It is estimated that about 10% of individuals with PD are in advanced stage, of whom only 10 – 30% receive an adequate treatment. The advanced therapies are expected to continue to grow for many years.
Currently available antiparkinsonian drugs allow an acceptable functional capacity during the early stages of PD. However, with advancing disease, it becomes increasingly difficult to counteract PD symptoms and side-effects despite optimised combinations of oral treatments. In the advanced stage, gastrointestinal dysfunction with erratic gastric emptying, short half-life of levodopa and a narrowing of the therapeutic window eventually result in a very compromised quality of life. As a consequence, most patients suffer from “On – Off” fluctuations. “On-off” fluctuations are sudden unpredictable shifts between “well-” or “over-” treated status (“On”) and an undertreated state with severe symptoms of parkinsonism (“Off”). These complications can be a major source of distress and disability and are difficult to treat. “Off”- time is of particular interest, as this is the biggest contributor to functional impairment in individuals with advancing PD.
A major goal in the treatment of advanced PD is therefore to provide continuous or continuous-like dopaminergic stimulation. Today, there are currently only three different continuous-like treatment options (device-aided therapies) available for people with advanced PD, see illustrations below:
At present, no direct comparative data support the use of one device-aided therapy over another. All treatments result in a significant reduction of the percentage of waking hours spent in ‘‘off’’ state. The choice of advanced therapy is probably best performed by a team of healthcare professionals with experience of all three advanced therapy options. The patient should be well informed about all available options and play a major part in decision-making.
Complete improvement of motor symptoms and dyskinesia is not obtained with any available treatment method. Each treatment has its own short and long-term risks and side effects. Thus, there are still unmet medical needs in the treatment of people with advanced PD.
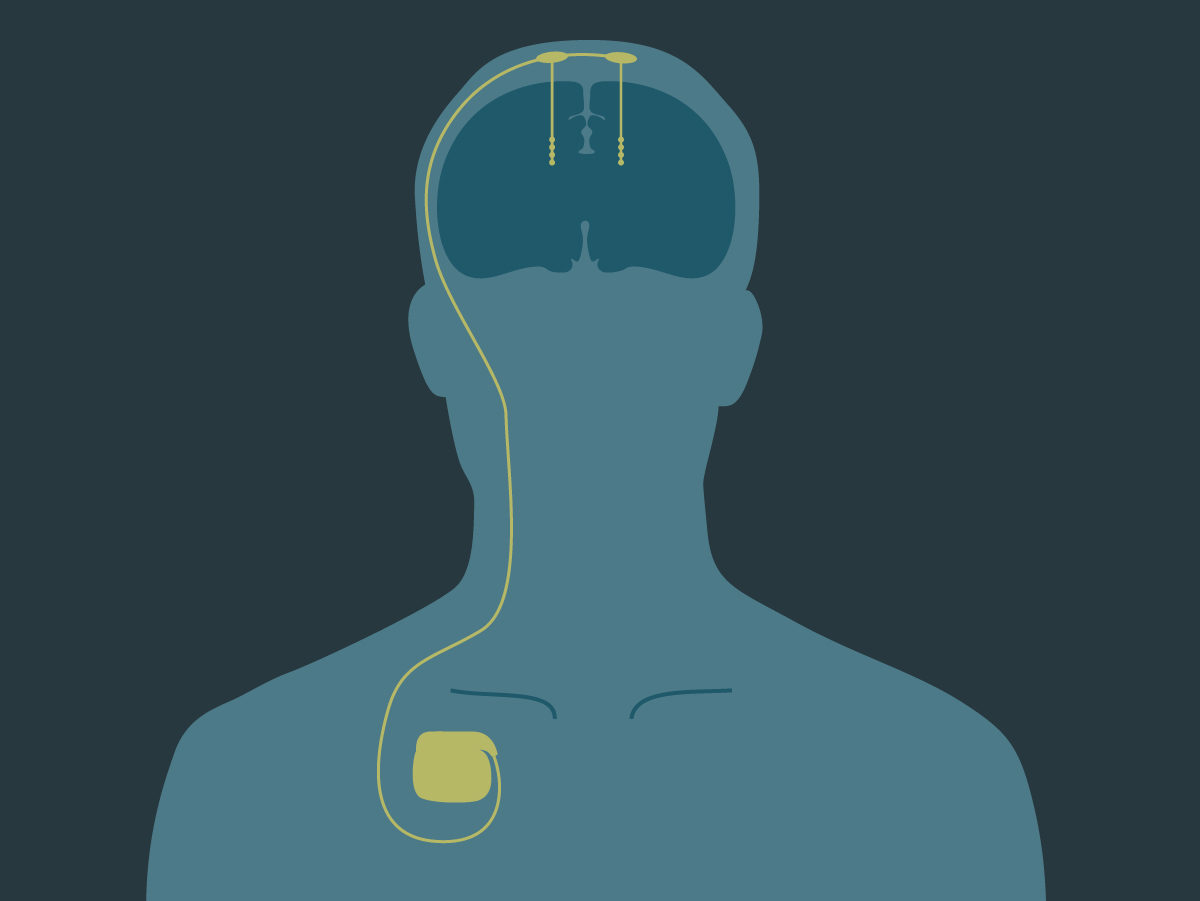
Deep brain stimulation (DBS)
DBS is a neurosurgical device involving the implantation of electrodes into the brain, which sends electrical impulses to specific targets in the brain (brain nuclei). Despite the long history of DBS, the underlying mechanisms are still not clear.
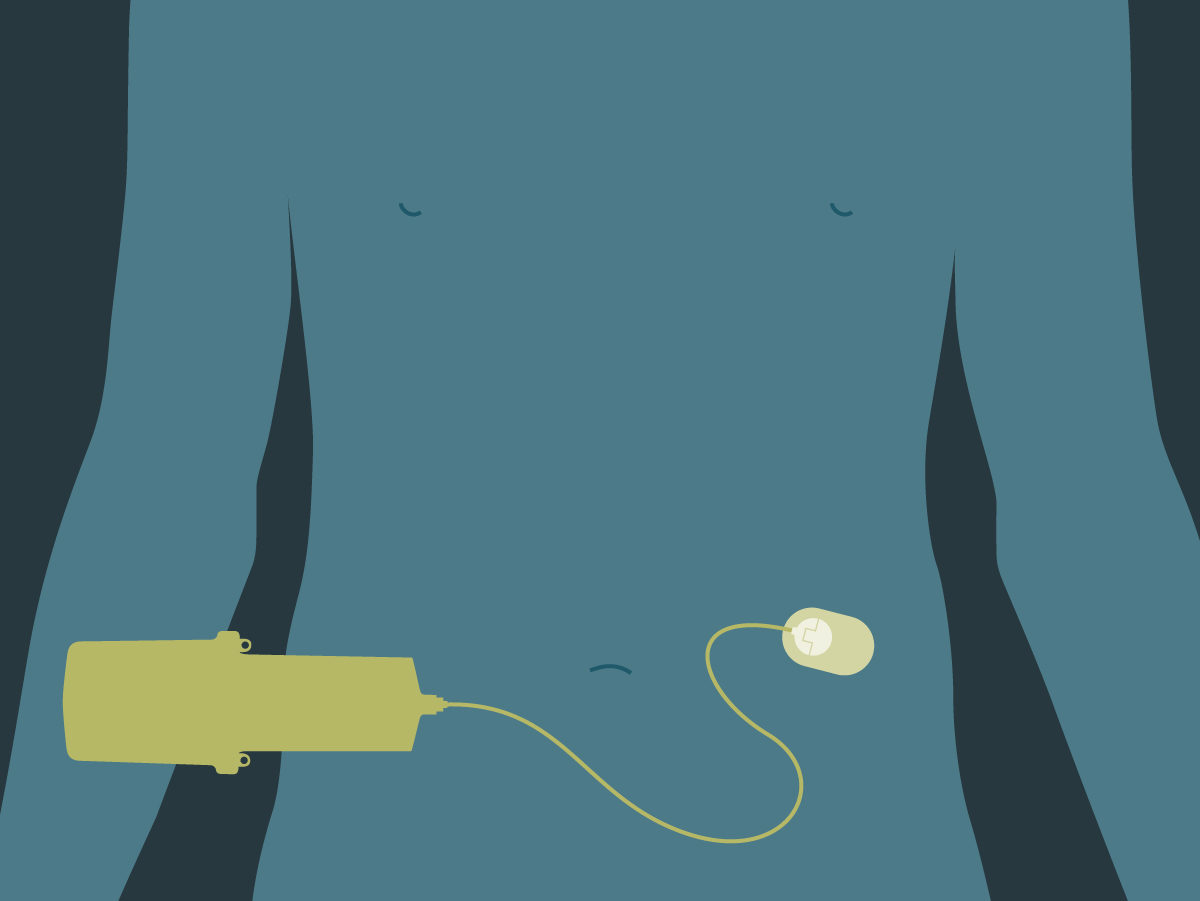
Continuous subcutaneous apomorphine
Apomorphine is a dopamine agonist, which mimics the action of the natural dopamine in the brain. Apomorphine is administered continuously, subcutaneously, with a pump.
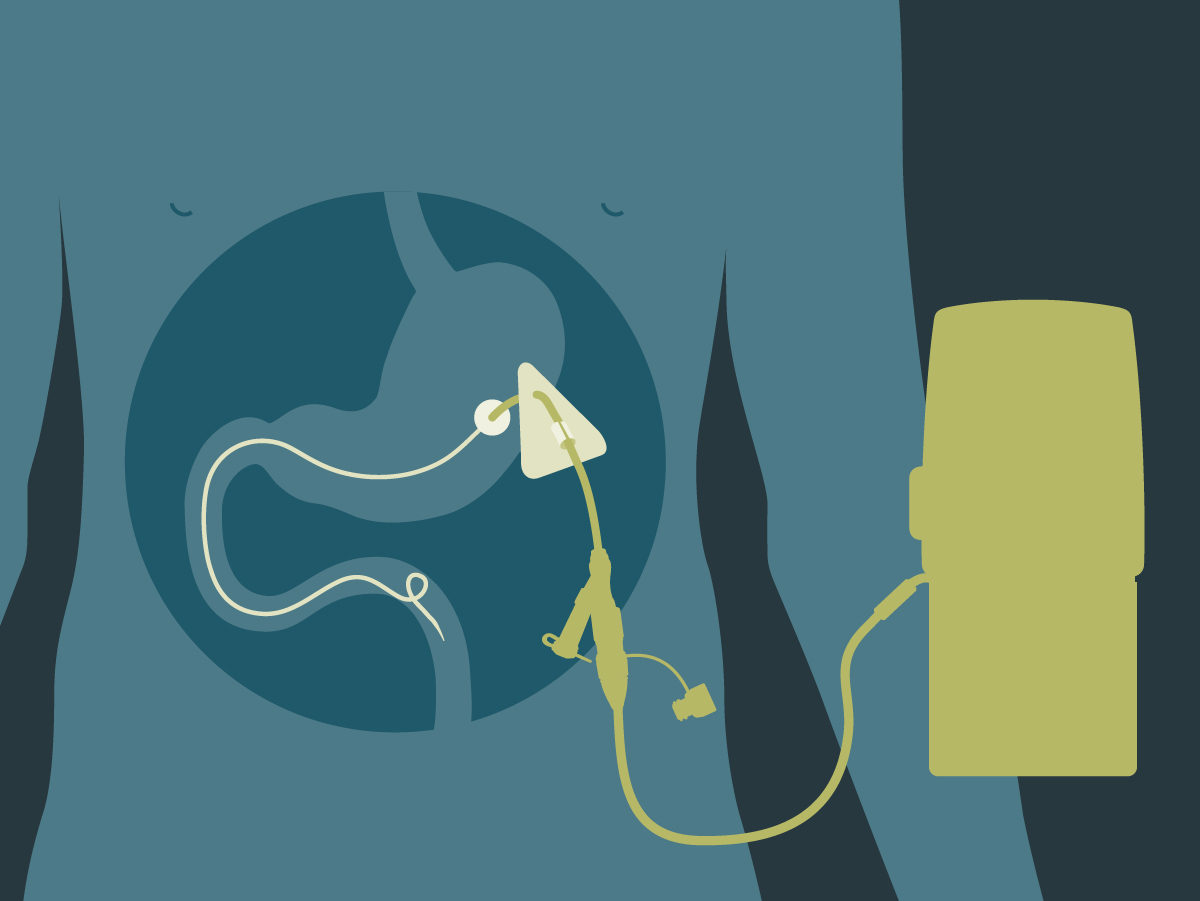
Levodopa-carbidopa intestinal gel (Duodopa)
Levodopa is converted into dopamine in the brain. Carbidopa, which inhibits peripheral metabolism of levodopa, is given to increase the bioavailability of levodopa. Duodopa is continuously administered intestinally through a tube with the help of an ambulatory pump.